中国寄生虫学与寄生虫病杂志 ›› 2026, Vol. 44 ›› Issue (1): 35-41.doi: 10.12140/j.issn.1000-7423.2026.01.006
樊羿辰1( )(
)( ), 张传山1, 侯娇2,3, 唐钊元1, 鲁雪梅1, 何荣东1, 加依达尔·胡玛尔汗1, 宋志浩1, 阚明轩1, 王明娟1, 孙立1, 温浩1,*()()
), 张传山1, 侯娇2,3, 唐钊元1, 鲁雪梅1, 何荣东1, 加依达尔·胡玛尔汗1, 宋志浩1, 阚明轩1, 王明娟1, 孙立1, 温浩1,*()()
FAN Yichen1()(), ZHANG Chuanshan1, HOU Jiao2,3, TANG Zhaoyuan1, LU Xuemei1, HE Rongdong1, JIAYIDAER Humaerhan1, SONG Zhihao1, KAN Mingxuan1, WANG Mingjuan1, SUN Li1, WEN Hao1,*()()
摘要:
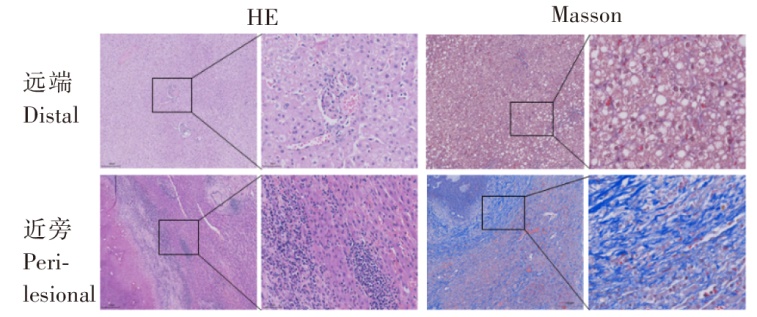
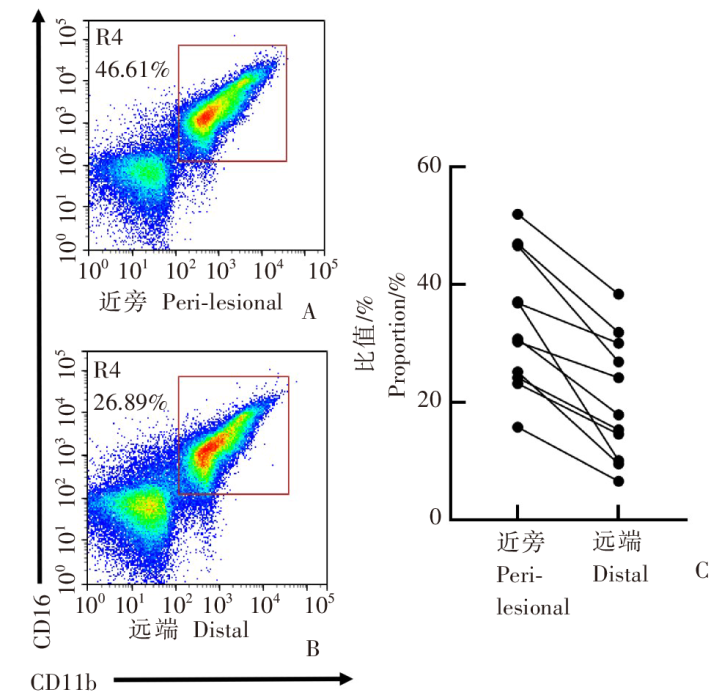
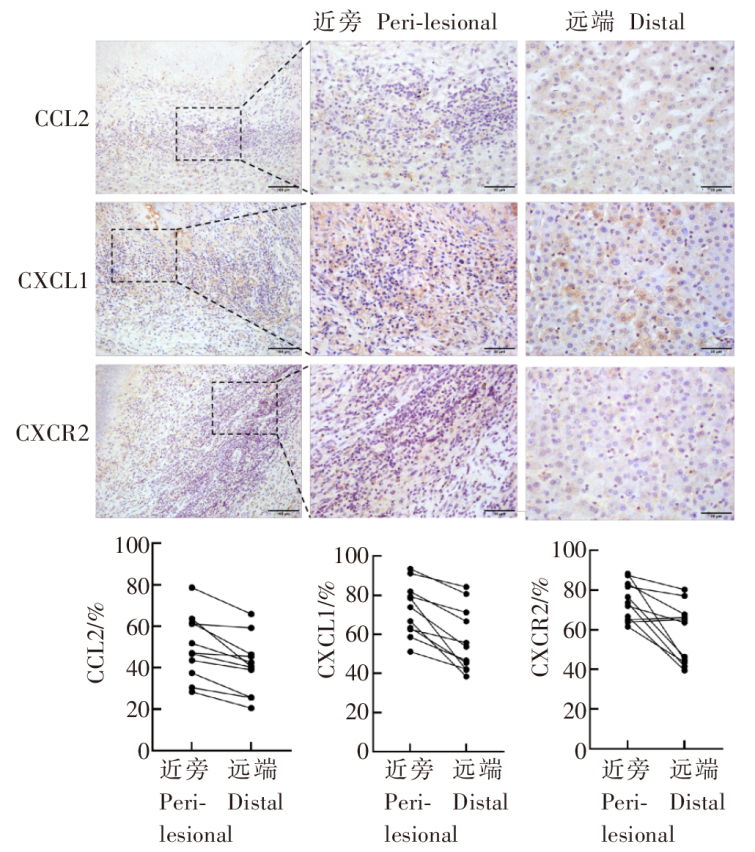
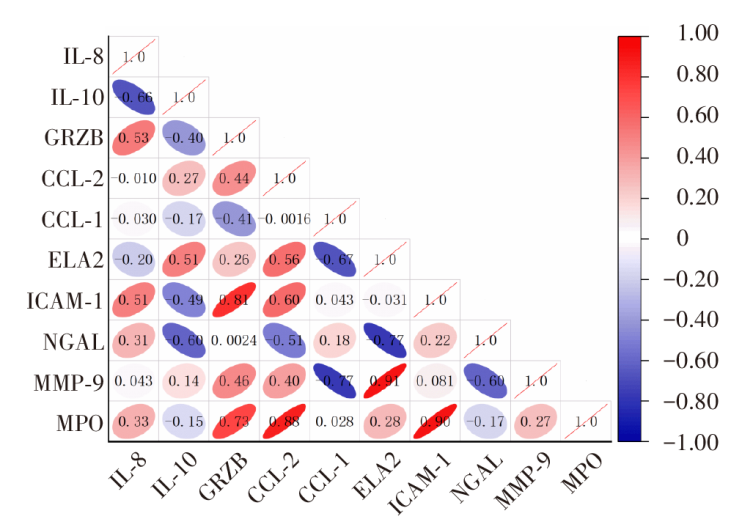
目的 探讨肝多房棘球蚴病(AE)患者外周血及肝脏中中性粒细胞水平、免疫微环境特征及其与疾病严重程度的关系。 方法 纳入2024年7月至2025年9月在青海大学附属医院接受手术治疗的24例AE患者(AE组)和24位健康者(HC组)为研究对象。AE组患者均经影像学与病理学确诊。收集研究对象性别、年龄、中性粒细胞计数、淋巴细胞计数、血小板计数、丙氨酸转氨酶(ALT)、天冬氨酸转氨酶(AST)数值,计算中性粒细胞与淋巴细胞比值(NLR)和系统免疫炎症指数(SII),对AE组进行PMN分型。使用GraphPad Prism 9软件分析AE组外周血临床指标间相关性。采集外周血与手术切除的病灶近旁及远端肝组织,行苏木精-伊红(HE)染色、Masson染色、免疫组织化学染色,使用QuPath-0.5.1软件分析2组趋化因子(C-C基元)配体2(CCL2)、趋化因子(C-X-C基元)配体1(CXCL1)、C-X-C基序趋化因子受体2(CXCR2)阳性区域面积占比。流式细胞术分析肝脏CD16⁺ CD66b⁺ 中性粒细胞水平及其与临床指标相关性。ELISA检测外周血与肝组织中白细胞介素8(IL-8)、IL-10、肿瘤坏死因子-α(TNF-α)、颗粒酶B(GRZB)、CCL2、弹性蛋白酶2(ELA2)、细胞间黏附分子-1(ICAM-1)、明胶酶相关脂质运载蛋白(NGAL)、基质金属蛋白酶(MMP-9)、髓过氧化物酶(MPO)等炎症因子的表达水平,并进行相关性网络分析。 结果 与HC组相比[(1.99 ± 0.62)× 109/L、(260.29 ± 40.36)× 109/L],AE患者外周血淋巴细胞和血小板水平下降[(1.60 ± 0.64)× 109/L、(229.75 ± 62.20)× 109/L](t = 2.036、2.018,均P < 0.05);ALT、AST、NLR、SII升高[AE组分别为(35.54 ± 27.53)U/L、(49.21 ± 47.63)U/L、2.06(区间1.48~3.27)、725.29(区间312.41~810.59),HC组分别为(24.17 ± 5.29)U/L、(49.20 ± 47.64)U/L、1.67 ± 0.37、420.58 ± 44.81](t = 2.319、2.604、2.317、2.051,均P < 0.05)。相关性分析显示,NLR、SII与PMN分型呈强正相关(r = 0.67,P < 0.01),与ALT呈弱正相关(P < 0.05)。病理学检查显示,与远端相比,病灶近旁存在严重的组织结构紊乱、肝细胞凝固性坏死和纤维化。流式细胞术检测结果显示,近旁CD16⁺ CD66b⁺ 中性粒细胞水平(20.49 ± 10.63)较远端(33.52 ± 11.23)显著升高(t = 6.923,P < 0.01),且与PMN分型呈正相关(r = 0.667,P < 0.05)。免疫组化显示CCL2、CXCL1、CXCR2在病灶近旁高表达(近旁分别为50.03 ± 15.30、72.77 ± 13.45、74.49 ± 10.55,远端分别为40.99 ± 13.78、56.94 ± 16.23、57.76 ± 15.26)(t = 6.492、5.527、3.747,均P < 0.05)。AE组外周血IL-6、IL-10、ELA2、NGAL、MMP-9、MPO和TNF-α水平升高;病灶近旁IL-8、IL-10、GRZB和CCL-2高表达,NGAL、MMP-9低表达。相关性网络分析结果显示,MPO与ICAM-1(r = 0.98)、MMP-9与ELA2(r = 0.88)呈极强正相关。 结论 AE患者肝病灶周围存在以趋化因子轴(CXCL1、CXCR2、CCL2)上调为驱动的中性粒细胞显著浸润。中性粒细胞通过释放氧化酶和基质降解酶的协同效应,驱动了病灶周围的炎症风暴与纤维化重塑。由局部免疫微环境恶化引发的病理改变,决定了疾病的严重程度(PNM分型),并同步映射外周血系统性炎症指标(NLR、SII)的显著升高。
中图分类号: