中国寄生虫学与寄生虫病杂志 ›› 2023, Vol. 41 ›› Issue (5): 644-646.doi: 10.12140/j.issn.1000-7423.2023.05.019
刘文虎1( ), 黄铭2, 梁金2, 刘建雄2,*, 温兆孟1, 马少波2
), 黄铭2, 梁金2, 刘建雄2,*, 温兆孟1, 马少波2
LIU Wenhu1(), HUANG Ming2, LIANG Jin2, LIU Jianxiong2,*, WEN Zhaomeng1, MA Shaobo2
摘要:
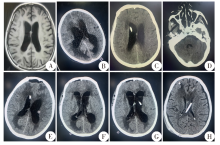
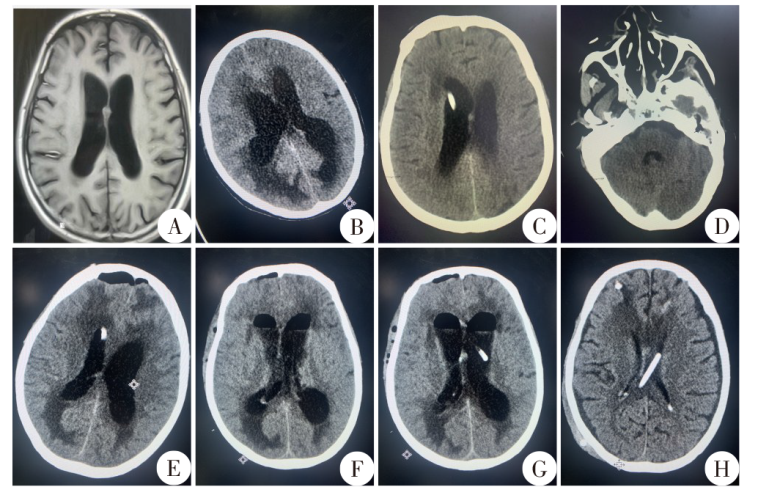
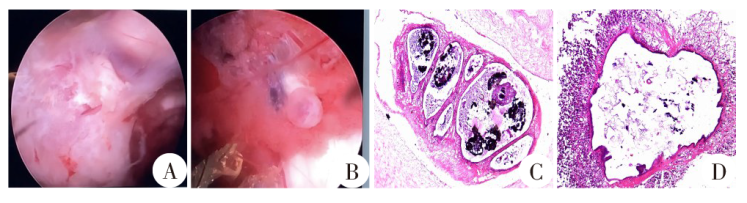
患者,男,53岁,农民,甘肃宕昌人。2021年11月19日因“头痛、头晕伴恶心、呕吐1周”就诊于甘肃省人民医院神经内科门诊。入院颅脑CT平扫示透明隔结节状稍高密度灶,头颅MRI示脑室轻度扩张。行腰椎穿刺术,颅内压180 mmH2O(1 mmH2O = 9.779 Pa);取脑脊液进行检测,总蛋白0.74 g/L。次日再行腰椎穿刺术,颅内压为300 mmH2O,遂转至神经外科作进一步治疗。患者颅压高,呈嗜睡状态,唤醒后不能正确对答,复查CT提示侧脑室扩张,考虑脑积水形成,存在脑疝风险。患者近年来有食未熟肉史,有肝棘球蚴病史。为降低患者颅压,11月26日行第1次脑室穿刺引流术,术后予重症监护。期间血清学检查提示猪囊尾蚴IgG抗体和弓形虫IgG抗体阳性,予吡奎酮(400 mg/8 h)和阿苯达唑(0.4 g/d)治疗3个疗程(7 d/疗程,疗程间隔5 d)。为改善患者脑积水症状,12月13日行第三脑室造瘘术(ETV),术后予驱虫治疗的同时行腰大池引流,但治疗效果不佳。12月28日和2022年1月11日行第2、3次脑室穿刺术以降低颅内压,术后驱虫治疗的同时予替加环素(50 mg/12 h)和舒普深(3 g/8 h)抗感染。1月25日患者颅内感染指标转阴,增强颅脑MRI未见明显脑囊尾蚴病灶。考虑堵管概率小,1月27日行脑室-腹腔分流术,术后患者意识清楚,复查头颅CT示脑室积水较前明显改善。患者于2月11日出院,出院时患者神志清楚,无明显头晕头痛、恶心呕吐和癫痫等症状。出院3个月后随访,患者病情恢复良好,生活可自理。
中图分类号: