中国寄生虫学与寄生虫病杂志 ›› 2019, Vol. 37 ›› Issue (2): 148-152.
宋世会, 桂希恩*( )
)
Shi-hui SONG, Xi-en GUI*()
摘要:
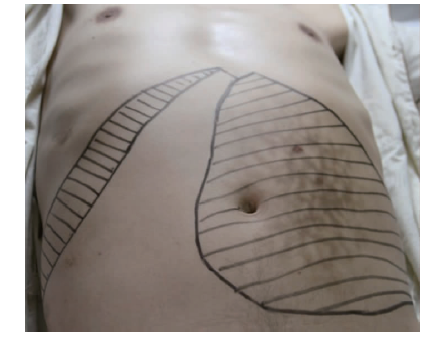
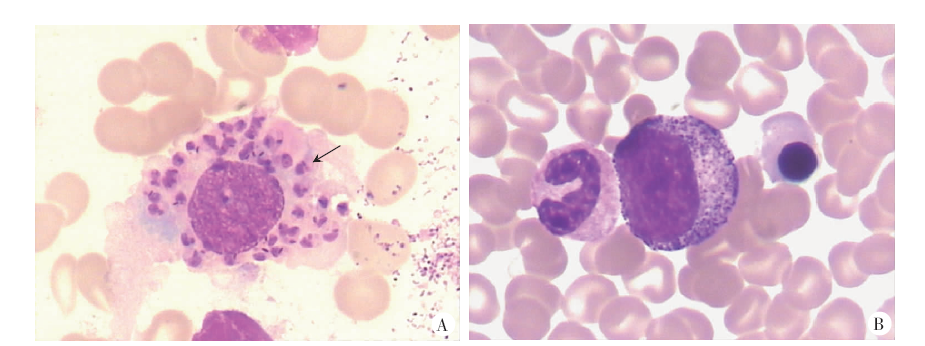
目的 报道使用葡萄糖酸锑钠长疗程治疗1例利什曼原虫与人类免疫缺陷病毒(HIV)合并感染患者的疗效及预后。方法 收集患者的临床资料,追踪观察患者的疗效及预后。结果 患者1990年在四川省九寨沟县(内脏利什曼病流行区)工作。1992年末出现发热、肝脾肿大,被多家医院诊断为“肝硬化”,对症治疗无效,脾脏持续肿大,并出现严重贫血、消瘦。1994年经骨髓穿刺涂片镜检发现利什曼原虫,诊断为内脏利什曼病,给予葡萄糖酸锑钠(五价锑600 mg/d × 6 d,静脉滴注)治疗,病情缓解。2010年8月,患者发现左上腹有包块,伴腹胀,再次行骨髓穿刺涂片镜检,发现利什曼原虫,再次给予葡萄糖酸锑钠(五价锑600 mg/d × 6 d,静脉滴注)治疗,病情缓解。住院期间初筛HIV抗体阳性,经蛋白质印迹(Western blotting)检测确认为HIV感染,CD4+ T淋巴细胞仅为42个/μl,诊断为艾滋病(AIDS)。2011年7月,患者开始接受抗HIV常规治疗[拉米夫定(3TC)300 mg/d + 齐多夫定(AZT)600 mg/d + 依非韦伦(EFV)600 mg/d],治疗2个月后出现严重贫血,将AZT更换为替诺福韦(TDF)300 mg/d,长期服用3TC + TDF + EFV。2012年7月25日患者因“腹胀2年”入住本院,入院时呈重度贫血貌,肝脏位于右锁骨中线肋缘下2 cm;脾脏下缘位于脐下7 cm,右缘位于前正中线右侧2 cm。骨髓涂片镜检查见利什曼原虫。继续给予抗HIV治疗(3TC + TDF + EFV),同时给予葡萄糖酸锑钠静脉滴注治疗内脏利什曼原虫感染[第1个疗程:先后给予葡萄糖酸锑钠(五价锑600 mg/d × 4 d,1 200 mg/d × 4 d)治疗,肝脾开始缩小后,改为隔天静脉滴注葡萄糖酸锑钠(五价锑600 mg/次 × 22次)]。在第1个疗程结束后1个月和3个月,分别给予1个疗程葡萄糖酸锑钠治疗(五价锑600 mg/次 × 18次)。3个疗程共计给予五价锑42 g治疗。2017年4月(抗利什曼原虫治疗结束后50个月)复诊,骨髓涂片检查未见利什曼原虫,CD4+ T淋巴细胞为249个/μl,HIV-RNA低于检测下限。结论 对内脏利什曼原虫合并HIV感染的患者给予葡萄糖酸锑钠长疗程及抗HIV治疗,内脏利什曼感染获得治愈,患者预后较好。
中图分类号: